Preclinical Research Services for Primary Biliary Cholangitis (PBC) and Cholestatic Liver Disease Models
Download
Driven by an autoimmune attack on the intrahepatic bile ducts, primary biliary cholangitis (PBC) is a progressive, immune-mediated cholestatic liver disorder characterized by chronic bile stasis, debilitating hepatic inflammation, and a high risk of progressing to cirrhosis or liver failure.
Protheragen offers a full spectrum of preclinical research solutions tailored to these complex hepatobiliary conditions. Our services include customized development of PBC and cholestatic liver disease models, from disease induction to phenotypic characterization, alongside integrated one-stop solutions covering diagnostic and therapeutic development, pharmacokinetics, and toxicology evaluations. This platform enables translational research that mirrors human disease progression and therapy responses.
Overview of Primary Biliary Cholangitis (PBC) and Cholestatic Liver Disease Models
Replicating the intricate etiology of human cholestatic disorders requires highly specialized in vivo systems that faithfully recapitulate chronic bile duct injury, localized immune dysregulation, and downstream fibrotic remodeling. Cholestatic liver disease models serve as indispensable translational bridges, utilizing genetic, chemical, surgical, or immunogenic induction methods to mirror the hallmark pathologies of PBC, such as antimitochondrial antibody (AMA) production, interlobular bile duct destruction, and progressive portal inflammation. These models provide a preclinical platform to interrogate the molecular mechanisms of biliary epithelial cell injury, assess portal immune cell infiltration, and evaluate the therapeutic potential of novel anticholestatic and antifibrotic drug candidates.
Applications of PBC and Cholestatic Liver Disease Models
Serving as a foundational pillar for translational hepatology, these robust disease models enable deep exploration of the mechanisms underlying biliary damage and accelerate the validation of next-generation therapeutics.
Pathophysiological Studies
Investigating the cellular signaling pathways governing bile acid toxicity, cholangiocyte apoptosis, and the breakdown of immune tolerance within the hepatic microenvironment.
Target Identification & Validation
Screening and confirming the therapeutic efficacy of novel biologics, small molecules, and gene therapies targeting specific receptors or immune checkpoints involved in biliary inflammation.
Biomarker Discovery
Identifying and profiling early circulating or imaging biomarkers associated with disease progression, including serum bile acid species, inflammatory cytokines, and non-invasive fibrosis metrics.
Preclinical Efficacy Screening
Providing high-resolution, reproducible readouts to evaluate the anticholestatic, anti-inflammatory, and antifibrotic performance of candidate compounds under clinically relevant conditions.
Workflow for PBC and Cholestatic Liver Disease Model Development
- Strategic Customization & Protocol Design: Aligning with specific therapeutic goals to select the optimal model induction strategy, and defining study timelines, cohort sizes, and baseline parameters.
- Model Induction & Real-Time Monitoring: Executing the chosen protocol under rigorous conditions, accompanied by continuous surveillance and physiological monitoring to ensure high survival rates and reliable disease onset.
- In Vivo Diagnostics & Biomarker Profiling: Performing longitudinal monitoring of disease progression via serum biochemistry (e.g., alkaline phosphatase, total bile acids, transaminases) and advanced in vivo imaging modalities to track structural changes in the liver.
- Histological & Molecular Validation: Conducting terminal evaluations using multiplex immunofluorescence, routine histology (Masson’s trichrome or Sirius Red for fibrosis assessment), and gene/protein expression profiling to confirm pathological features consistent with human disease.
- Data Delivery and Reporting: Compiling a comprehensive data package featuring detailed statistical analysis, high-resolution digital pathology images, and a meticulous final report suitable for regulatory submissions and strategic decision-making.
Available PBC and Cholestatic Liver Disease Animal Models
| Model | Strain | Application |
|---|---|---|
| 2OA-BSA Induced Model | C57BL/6 Mice | Investigating disease initiation, breakdown of immune tolerance, AMA production, and evaluating immunomodulators or targeted autoimmune therapies. |
| 2OA-BSA + Poly I:C Immunized Model | C57BL/6 Mice | Investigating innate immune amplification in PBC; evaluating therapeutics targeting the Th1/Th17 pathway, innate immunity, or advanced/fibrotic stages of PBC. |
| ANIT Induced Model | SD Rat, C57BL/6 Mice | Studying chronic cholestatic injury and fibrosis, evaluating anti-cholestatic and anti-fibrotic agents, and testing bile acid transporter/FXR/PPAR agonists. |
| Bile Duct Ligation (BDL) Model | SD Rat | Studying advanced biliary cirrhosis, portal hypertension, and secondary obstructive liver injury; evaluation of anti-fibrotic agents (not suitable for studying disease initiation). |
Integrated Preclinical Research Services for PBC and Cholestatic Liver Disease
Synthesizing all phases of development into an optimized, multi-disciplinary preclinical service pipeline allows for seamless data continuity and rapid asset advancement.
Engineers and validates novel diagnostic modalities including high-affinity antibodies for serum biomarkers, custom assays for AMA detection, and functional molecular probes for non-invasive, high-resolution imaging of the biliary tract.
- Omics Analysis
- Biomarker Analysis
- And More
Supports early-stage discovery through high-throughput screening, custom cholangiocyte-immune cell co-culture assays, and in vivo pharmacology testing to evaluate target engagement and downstream therapeutic responses.
Delivering proprietary and customized chemical, surgical, or genetically engineered mouse and rat platforms precisely tailored to mirror specific sub-phenotypes or distinct stages of biliary disease progression.
Conducts rigorous bioanalytical profiling, tissue distribution tracking, and safety margin evaluations complemented by detailed liver histopathology and systemic toxicity panels to clear safety hurdles ahead of IND filings.
Case Study 01- 2OA-BSA Induced Model
Female C57BL/6 mice were immunized with 2-octynoic acid conjugated to bovine serum albumin (2OA-BSA) emulsified in complete Freund’s adjuvant (CFA) to break immune tolerance to the self-antigen lipoylated PDC-E2 via molecular mimicry. This induction method generated a PBC-like phenotype characterized by progressive bile duct damage.
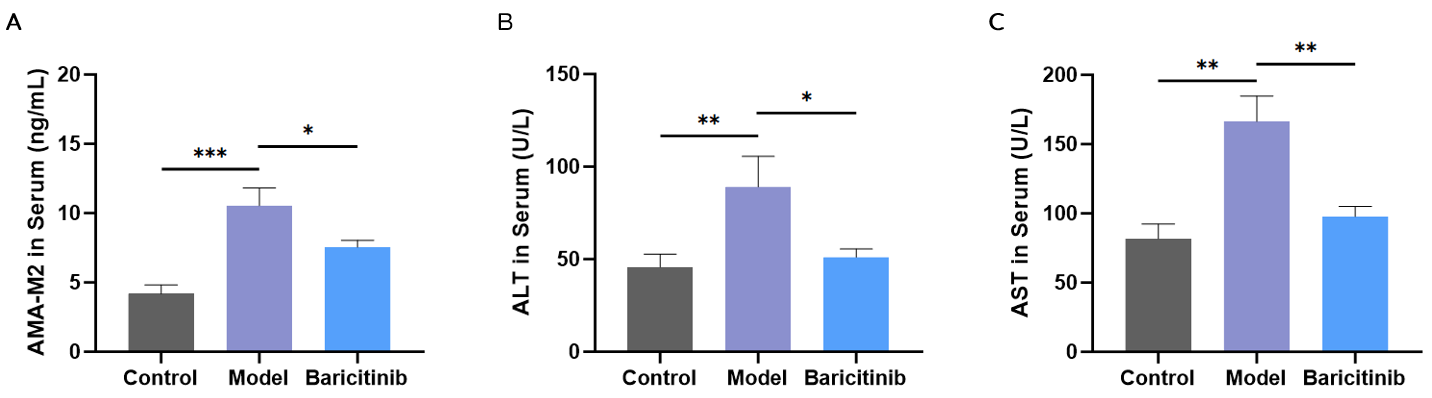
Fig.1 Serum AMA-M2, ALT, and AST levels. The model group showed elevated AMA-M2 titers, ALT, and AST versus controls; Baricitinib reduced these elevations. Data are presented as mean ± SEM (n=10; ***p < 0.001, **p < 0.01, *p < 0.05).
Body weight changes and elevated serum pro-inflammatory cytokines (TNF-α, IFN-γ) were observed in the immunized mice compared to controls. Histopathological examination revealed bile duct inflammation and portal tract infiltration, recapitulating key human PBC features. The model group showed marked increases in serum AMA-M2, ALT, and AST, as well as elevated spleen and liver weights. In contrast, the Baricitinib-treated group exhibited attenuated elevations in these parameters, indicating a suppressive effect on immune-mediated biliary injury. This model provided a robust platform for preclinical efficacy testing of immunomodulatory and anti-cholestatic therapeutics.
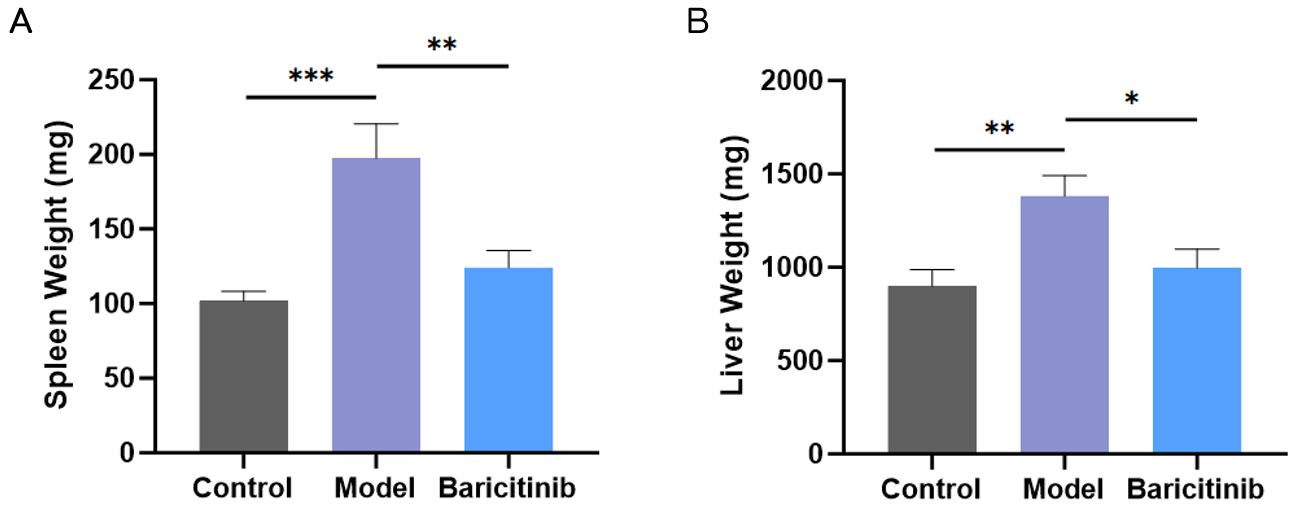
Fig.2 Spleen and liver weights. Both organ weights were higher in the model group than in controls, indicating immune activation and hepatomegaly; Baricitinib reduced both parameters. Data are presented as mean ± SEM (n=10; ***p < 0.001, **p < 0.01, *p < 0.05).
Case Study 02- 2OA-BSA + Poly I:C Immunized Mouse Model
C57BL/6 mice were immunized using a multi-factor protocol consisting of 2OA-BSA, polyinosinic-polycytidylic acid (Poly I:C), and pertussis toxin (PTX) over 12 to 16 weeks (3 to 4 cycles). Animals were assigned to three groups: control (vehicle), model (induction + vehicle), and Cyclosporine A (induction + Cyclosporine A therapy). The model group showed elevated serum alkaline phosphatase (ALP), total bilirubin (T-BIL), and alanine aminotransferase (ALT) compared to controls, indicating cholestatic hepatic injury. Cyclosporine A therapy reduced these elevations relative to the model group.
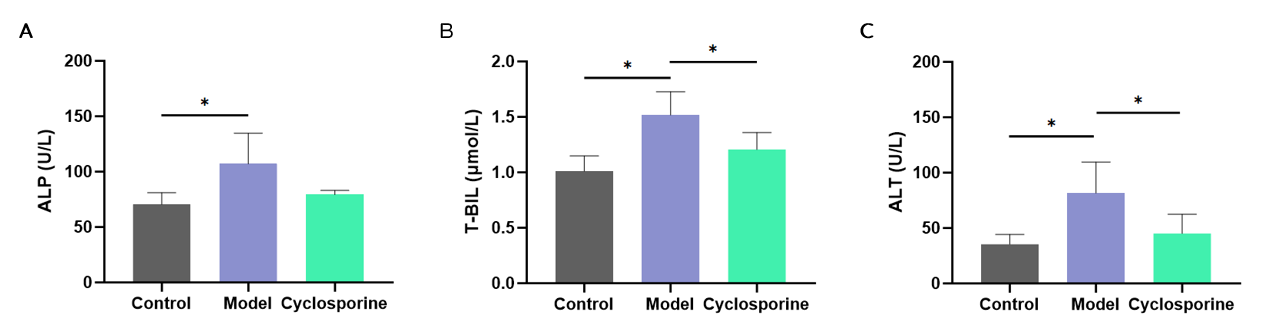
Fig.3 Serum ALP, T-BIL, and ALT levels in control, model, and Cyclosporine A-treated groups. The model group exhibited increased levels of all three markers compared to controls, and Cyclosporine A therapy attenuated these increases. Data are presented as mean ± SEM (n=10; *p < 0.05).
Case Study 03- ANIT Induced Model
ANIT was administered to SD rats by oral gavage at 100 mg/kg once weekly for 4 consecutive weeks (4 doses total). Animals were divided into three groups: control (vehicle), model (ANIT + vehicle), and positive control therapy (ANIT + UDCA). The model group exhibited decreased body weight kinetics and elevated serum levels of ALT, AST, ALP, total bilirubin, direct bilirubin, and indirect bilirubin at endpoint compared to controls. Increased liver and spleen weights, along with higher liver and spleen indices, were observed in the model group. Histopathological examination revealed bile duct lesions and periductal fibrosis. UDCA therapy attenuated these biochemical, organ weight, and histopathological alterations relative to the model group.
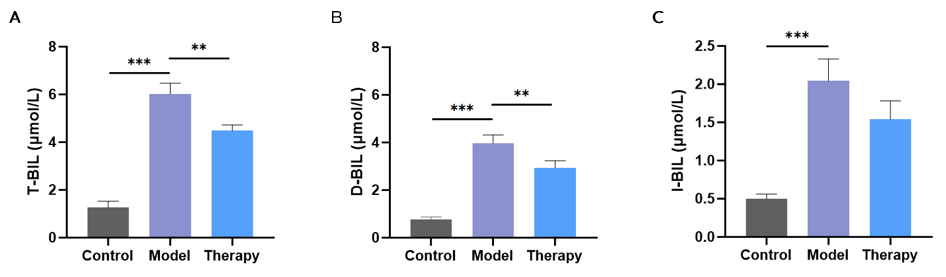
Fig.4 Serum total bilirubin (T-BIL), direct bilirubin (D-BIL), and indirect bilirubin (I-BIL) levels in control, model, and UDCA-treated groups. The model group showed marked elevations in all three markers compared to controls, indicative of ANIT-induced cholestatic injury. UDCA therapy reduced these elevations. Data are presented as mean ± SEM (n=10; ***p < 0.001, **p < 0.01).
Why Choose Us?
- Translational Rigor and Precision: Utilizing highly validated, mechanism-specific models that accurately replicate human pathology, ensuring high predictability for translation into human clinical trials.
- End-to-End Solution: Delivering a seamless, integrated service continuum that consolidates diagnostic innovation, bespoke disease modeling, advanced pharmacology, and safety testing under one roof to maximize efficiency and data continuity.
- Deep Scientific and Hepatology Expertise: Backed by an elite team of biopharma-experienced pathologists, immunologists, and hepatologists dedicated to optimizing study designs and providing nuanced data interpretation.
- High Quality Data and Reproducibility: Maintaining stringent standard operating procedures, advanced bioanalytical platforms, and robust quality control metrics to deliver decision-enabling, audit-ready data packages.
Contact Us
Navigating the complexities of biliary autoimmune disorders requires an experienced partner with deep domain expertise and robust model systems. Protheragen offers customized disease models, efficacy and safety testing, and integrated diagnostics and therapeutic development services, all under one-stop preclinical platform. To learn more about our specialized model portfolios, customized validation protocols, or to discuss integrating your therapeutic candidate into our testing pipelines, please reach out to our scientific consultation team.
All of our services and products are intended for preclinical research use only and cannot be used to diagnose, treat or manage patients.